SOLID PSEUDOPAPILLARY TUMOR OF PANCREAS “FRANTZ TUMOR” CASE REPORT AND REVIEW TUMOR PSEUDOPAPILAR SÓLIDO DEL PÁNCREAS “TUMOR DE FRANTZ” INFORME DE CASO Y REVISIÓN
Pablo Magaña Mainero1, Valeria Hernández Luna2, Ismael Domínguez Rosado3, Luis Carlos Chan-Núñez4
1. General Surgery, Centro Médico ABC. Correo: lunavle14@gmail.com
2. Liver-Pancreatic-Biliary Surgery
3. Chief of Liver-Pancreatic-Biliary Surgery,
Instituto Nacional de Ciencias Médicas y Nutrición
Salvador Zubirán
4. Hospital Ángeles Centro Sur
5. Faculty of Medicine, UNAM
ABSTRACT
The solid pseudopapillary pancreatic tumor, also called “Frantz
tumor”, was first described in 1959 by Dr. Frantz Gruber. Part of
the classification of cystic neoplasms of the pancreas, it is a
condition presented predominantly in young women, with a frequency of
90% of cases.
A 24-year-old female patient complained of abdominal pain for 3 days,
accompanied by nausea, vomiting, and abdominal distention. A
double-contrast and a PET scan were performed that identified a lesion
with a solid aspect in the pancreatic tail and in the liver segments
VIII and V.
A subtotal pancreatectomy with splenectomy and biopsy of liver lesions
was performed, reporting positive for malignancy. It was decided to
perform a right portal vein ligation. On the eighth postoperative day,
right-sided two-stage hepatectomy was completed. On the first
postoperative day of the second surgery, she presented clinical signs
compatible with bleeding, confirmed with tomography as a hematoma in
the surgical bed. Exploratory laparotomy was performed with hematoma
drainage. She went to an Intensive Care Unit, where she evolved without
complications. Postoperative bleeding in patients with hepatectomy
varies from 4.2% to 10%, and there are several reasons for its
occurrence. In our case, the diagnosis and control of bleeding on the
surface of the resection were accurately performed. Postoperative
bleeding is one of the most frequent operative complications of
hepatectomy, so it is necessary to bring it under control.
Key words: Pancreatic neoplasm, Frantz tumor, metastasis, portal vein ligation, hepatectomy
Tumor pseudopapilar sólido del páncreas “tumor de Frantz” Informe de caso y revisión
RESUMEN
El tumor pancreático pseudopapilar sólido, también
llamado “Tumor de Frantz”, fue descrito por primera vez en
1959 por el Dr. Frantz Gruber. Forma parte de la clasificación
de las neoplasias quísticas del páncreas y se presenta
predominantemente en mujeres jóvenes, hasta en el 90% de los
casos. Una paciente de 24 años, con dolor abdominal de 3
días de evolución, acompañado de náuseas,
vómitos y distensión abdominal. Se le realizó una
tomografía computarizada que identificó una lesión
con aspecto sólido del parénquima pancreático a
nivel de la cola, y lesiones hepáticas en los segmentos VIII y
V. Se le practicó una pancreatectomía subtotal con
esplenectomía y una biopsia de las lesiones hepáticas,
que resultó positiva para malignidad. Se decidió realizar
una ligadura de la vena porta derecha. En el octavo día
postoperatorio, se completó una hepatectomía derecha en
dos etapas. En el primer día postoperatorio de la segunda
cirugía, presentó signos clínicos compatibles con
hemorragia, que se confirmó mediante tomografía
computarizada como un hematoma en el lecho quirúrgico. Se
realizó una laparotomía exploratoria con drenaje del
hematoma. La paciente fue trasladada a la Unidad de Cuidados
Intensivos, donde evolucionó sin complicaciones. El sangrado
posoperatorio en pacientes sometidos a hepatectomía varía
entre el 4,2 % y el 10 %, y las causas descritas son diversas. En
nuestro caso, en relación con el sangrado en la superficie de la
resección, el diagnóstico y el control se realizaron
correctamente. El sangrado posoperatorio quirúrgico es una de
las complicaciones operatorias más frecuentes de la
hepatectomía, por lo que es necesario tenerlo en cuenta y no
demorar su tratamiento para un control definitivo.
Palabras clave: Neoplasia pancreática, tumor de Frantz, metástasis, ligadura de la vena porta, hepatectomía
INTRODUCTION
The solid pseudopapillary tumor of the pancreas (SPT) also called
“Frantz’s tumor” was first described in 1959 by Dr.
Frantz Gruber, however, it was in 1970 when Hamoudi described the
histopathology and until 1980 that Kloppel described it as a particular
clinical entity. In 1996 the World Health Organization (WHO) defined it
as “Pseudopapillary solid neoplasm” (1).
This tumor belongs to the classification of pancreatic cystic
neoplasms, being the least common, with an incidence of 1–3%
among them. It predominantly affects young women in 90% of cases, with
a mean age of 22 years (range: 20–30 years), although it has also
been reported in men (mean age: 37 years) and children (under 12 years
old) (1,2). The average size ranges from 6 to 8 cm, but some cases
reach diameters of 15 to 22 cm (7). Furthermore, although it presents a
low risk of malignancy, up to 15% of patients may develop metastases
(8). SPT has been associated with mutations in exon 3 of CTNNB1 and
alterations in Wnt/B-catenin and Hedgehog signaling pathways (7).
In this context, the ALPPS technique (Associating Liver Partition and
Portal vein Ligation for Staged Hepatectomy) first described in 2012
(9), is designed to rapidly increase the volume of the future remnant
liver (FRL), allows liver resections in two stages (9) It combines two
established procedures: right portal vein ligation (PVL), which
restricts blood flow to a portion of the liver, and in situ liver
splitting, which allows for enhanced regeneration of the organ to
facilitate resection of the remaining portion (11).
ALPPS-induced liver regeneration is mainly attributed to portal
hemodynamic alterations rather than to circulating proliferative
factors. Hepatic transection and portal ligation generate an increase
in portal flow in the FLR, which increases portal pressure and
stimulates hepatocyte hypertrophy, reaching a growth of 65% to 110% in
an interval of 6 to 15 days. This process involves the activation of
signaling pathways such as JNK1-IHH, the production of nitric oxide by
the sinusoidal endothelium and the induction of hypoxia in the FLR,
which enhances cell proliferation. In experimental models, an increase
of 60% in 24 hours and up to 134% in 72 hours has been reported. In
addition, hepatic transection disrupts porto-portal collaterals,
preventing venous outflow leakage and ensuring a more effective
regenerative stimulus. These findings suggest that regeneration in
ALPPS is predominantly driven by changes in hepatic hemodynamics and
sinusoidal microcirculation, rather than by cytokines or growth factors
(10).
ALPPS has been used mainly in patients with bilobar liver metastases or
primary liver tumors initially considered unresectable, achieving
success rates close to 99% in the second stage (9).
On the other hand, there are different types of ALPPS that are applied
according to the clinical situation of the patient, including Classic
ALPPS, which involves complete transection of the hepatic parenchyma
and ligation of the portal vein, and Partial ALPPS, with partial
transection of the parenchyma and ligation of the portal vein. Mini
ALPPS is characterized by partial parenchymal transection and portal
vein embolization through the inferior mesenteric vein. In addition,
Hybrid ALPPS combines complete transection with an anterior approach
and two-stage portal embolization. Finally, Modified ALPPS preserves
the portal pedicles during liver transection (9).
The accelerated hepatic regeneration promoted by the ALPPS technique
allows complete resection in a shorter period of time, usually between
7 and 15 days between surgical stages; however, this technique also
entails an increase in postoperative morbidity (9).
We are dealing with an infrequent entity with an even rarer
presentation, so we consider it important to present the case and a
review of the subject with the complications associated with surgical
treatment.
CASE PRESENTATION
24-year-old female patient, with a history of peptic acid disease of 2
years of evolution under control with medical treatment and irritable
bowel syndrome under control. She started her symptoms with abdominal
pain of 3 days of evolution, of transictal type in the epigastrium of
intensity 7/10, accompanied by nausea, vomiting and abdominal
distension. On physical examination there were no specific findings,
the initial laboratories were within normal parameters, so imaging
studies were performed.
Investigations and Examinations
Double contrast tomography identified a solid-cystic lesion of the
pancreatic parenchyma at the level of the tail with dimensions of 62 x
75 x 70 mm. In addition, in the liver there were lesions in segment
VIII of 13 mm and segment V of 16 and 12 mm (Figure 1).
The patient was admitted to complete the study protocol, PET CT was
requested and reported a lesion in the tail of the pancreas, of
heterogeneous density, solid, with lobulated and well-defined border,
measuring 67 x 83 mm in its major axes, associated with metabolism with
a maximum SUV of 14.5. The liver with multiple hypodense lesions in
segments V, VI, VII and VIII, the largest lesion in segment 6,
measuring 17 mm, and associated with increased metabolism with maximum
SUV of 7.1, with splenomegaly (Figure 3). Tumor markers were requested,
which were reported in normal ranges; Carcino Embryonic Antigen of 5,
Alpha-feto protein of 1.1, Ca 19.9 of 2. Subsequently, an endoscopic
ultrasound biopsy was performed, which reported a solid pseudopapillary
tumor of the pancreas (TSP), so she was scheduled for surgery.
Treatment
She was scheduled for subtotal pancreatectomy with splenectomy (Figure
4), biopsy of hepatic lesions in segments IV, VI, VII reported positive
for malignancy so it was also decided to perform ligation of the right
portal vein. Without complications.
The pathology reported: Pancreas; solid pseudopapillary carcinoma
without neoplasia in surgical edge. Liver biopsy; solid pseudopapillary
carcinoma metastatic in two hepatic wedges.
RESULTS
On the 8th postoperative day a right hepatectomy was performed and the
transoperative findings were reported; Hypertrophy of the left hepatic
lobe with metastasis of pseudopapillary carcinoma of the pancreas
limited to the right liver, without evidence of invasion by
transoperative ultrasound.
On the first postoperative day of the second procedure, she presented
with hemorrhage confirmed by tomography (Figure 2) as a hematoma in the
surgical site. She underwent exploratory laparotomy in which a 1300 ml
hematoma drainage and hemostasis of the surgical site was performed.
She was transferred to the Intensive Care Unit due to past reports of
hemorrhage and for close monitoring, she evolved without complications
and was discharged on the ninth postoperative day.
DISCUSSION
Solid pseudopapillary tumor of the pancreas is a rare tumor and
requires surgery for its treatment. Among its frequent postoperative
complications are biochemical leakage and pancreatic fistula,
peripancreatic collections and abscesses, hemorrhage and hematoma,
pancreatic pseudocyst, intestinal occlusion, cholangitis and surgical
wound infection (3).
Postoperative bleeding in hepatectomy patients ranges from 4.2-10%, and
the described reasons for its occurrence are threefold: 1) bleeding
from the resection surface, 2) incomplete hemostasis in the
transoperative period, and 3) loss of tension or release of vascular
staples or sutures (4, 5).
In this case, the hemorrhage was related to the first cause described,
was diagnosed and optimally controlled. It is increasingly feasible to
diagnose and treat these tumors at a wider range of stages, however,
complications arising from pancreatic and hepatic resections represent
a significant challenge for the surgeon and the medical team. The
morbidity and mortality of these patients can increase rapidly, so
these procedures should be performed in specialized centers by a
multidisciplinary team with experience in the management of these
complications.
Hepatopancreatectomies are highly complex procedures that require
meticulous surgical planning. In this case, in order to optimize the
hypertrophy of the future remnant liver (FLR) and to allow a safe
two-stage resection, we chose to perform a Mini-ALPPS, a modified
variant of the classic ALPPS. Unlike the latter, where hepatic
transection is complete in the first stage, Mini-ALPPS employs partial
parenchymal transection and portal vein embolization to stimulate
hepatic hypertrophy in a more controlled manner, avoiding extensive
manipulation of the hepatic hilum and reducing the physiological impact
of the procedure (12).
In previous studies, it has been shown that liver regeneration in
Mini-ALPPS occurs mainly due to hemodynamic changes that increase
portal flow to the FLR, favoring a more rapid hypertrophy than that
observed in conventional techniques such as portal embolization (12).
However, although Mini-ALPPS allows accelerated liver regeneration, it
has also been reported that it may be associated with higher
postoperative morbidity and mortality compared to less invasive
techniques, particularly in patients with advanced liver fibrosis (12).
In comparison with other reports of Mini-ALPPS, in this case we were
able to complete the resection in two times with adequate FLR growth
and without major postoperative complications. These findings reinforce
the usefulness of this technique in patients with liver metastases from
pancreatic tumors, in whom the remaining liver volume may be a limiting
factor for complete oncologic resection (12).
CONCLUSION
Frantz tumor is a rare entity, with greater frequency in young women,
surgery resection with free margins is the therapeutic option of
choice. Routine lymphadenectomy has not proven to be useful. Metastases
of this tumor are present in 20% of the cases at the time of diagnosis
and the cases in which a resection of these metastases can be performed
in the same surgical time are exceptional (6).
The frequency of complications faced peri-operatively due to resection
of the primary tumor in the pancreas or metastases in the liver have a
direct influence on the patient’s prognosis.
AUTHORS’ CONTRIBUTIONS
All authors contributed substantially to the development of this
manuscript. Case conception, data collection, literature review, and
drafting of the report were shared responsibilities. All authors
reviewed and approved the final version of the manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest related to this publication.
REFERENCES
1. Dinarvand P, Lai J. Solid Pseudopapillary Neoplasm of the
Pancreas: A Rare Entity With Unique Features. Arch Pathol Lab Med.
2017;141(7):990–5.
2. Fasanella KE, McGrath K. Cystic lesions and intraductal neoplasms of
the pancreas. Best Pract Res Clin Gastroenterol. 2009;23(1):35–48.
3. Romics L, Oláh A, Belágyi T, Hajdú N, Gyurus P,
Ruszinkó V. Solid pseudopapillary neoplasm of the
pancreas—proposed algorithms for diagnosis and surgical
treatment. Langenbecks Arch Surg. 2010;395(6):747–55.
4. Jin S, Fu Q, Wuyun G, Wuyun T. Management of post-hepatectomy
complications. World J Gastroenterol. 2013;19(44):7983–91.
5. Russell MC. Complications following hepatectomy. Surg Oncol Clin N Am. 2015;24(1):73–96.
6. Reddy S, Cameron JL, Scudiere J, Hruban RH, Fishman EK, Ahuja N, et
al. Surgical management of solid-pseudopapillary neoplasms of the
pancreas (Franz or Hamoudi tumors): a large single-institutional
series. J Am Coll Surg. 2009;208(5):950-7.
7. Zalatnai A, Kis-Orha V. Solid-pseudopapillary neoplasms of the
pancreas is still an enigma: a clinicopathological review. Pathol Oncol
Res. 2020;26(2):641–9.
8. Printes TRM, de Castro GL, Rabelo DC, da Silva Neto RA, da Silva
Junior RA. Frantz’s tumor as incidental finding during Heller
myotomy for achalasia: case report and review of literature. Ann Med
Surg (Lond). 2024;86(8):4861–4.
9. Memeo R, Conticchio M, Deshayes E, Nadalin S, Herrero A, Guiu B, et
al. Optimization of the future remnant liver: review of the current
strategies in Europe. Hepatobiliary Surg Nutr. 2021;10(3):350–63.
10. Zhang S, Ma Y, Chen X, Wu S, Chen G. Circulating proliferative
factors versus portal inflow redistribution: mechanistic insights of
ALPPS-derived rapid liver regeneration. Front Oncol. 2025;14:1429564.
11. Balci D, Sakamoto Y, Li J, Di Benedetto F, Kirimker EO, Petrowsky
H. Associating liver partition and portal vein ligation for staged
hepatectomy (ALPPS) procedure for cholangiocarcinoma. Int J Surg.
2020;82(Suppl):97–102.
12. Liu GM, Zhang YM. Mini-ALPPS-based multidisciplinary treatment
leading to long-term survival in a patient with a large HCC: a case
report. Front Surg. 2023;9:920953.
13. Eshmuminov D, Raptis DA, Linecker M, Wirsching A, Lesurtel M,
Clavien PA. Meta-analysis of associating liver partition with portal
vein ligation and portal vein occlusion for two-stage hepatectomy. Br J
Surg. 2016;103(13):1768–82.
14. Lang H, Baumgart J, Mittler J. Associated liver partition and
portal vein ligation for staged hepatectomy (ALPPS) registry: what have
we learned? Gut Liver. 2020;14(6):699–706.
15. Schnitzbauer AA, Lang SA, Goessmann H, Nadalin S, Baumgart J,
Farkas SA, et al. Right portal vein ligation combined with in situ
splitting induces rapid left lateral liver lobe hypertrophy enabling
2-staged extended right hepatic resection in small-for-size settings.
Ann Surg. 2012;255(3):405–14.

Figure 1. Double contrast CT-Scan identified a solid-cystic lesion on
the pancreatic parenchyma at tail’s level, measuring 62 x 75 x 70
mm, with heterogeneous reinforcement and mass effect towards the
greater curvature of the stomach and involvement of splenic arterial
and venous branches with engorgement and collateralization of its
branches. In addition, the liver showed solid hypodense lesions with
diffuse heterogeneous reinforcement during the contrasted phases
suggestive of secondary deposits; in segment VIII of 13 mm and segment
V of 16 mm and 12 mm
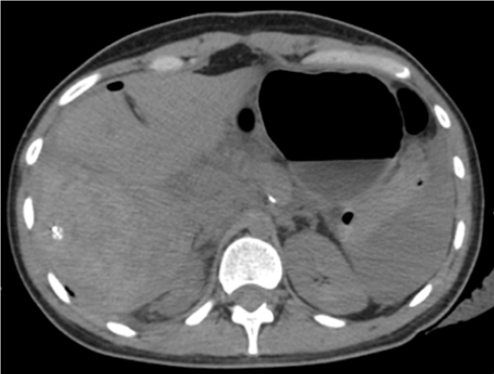
Figure 2. Extensive hematoma is observed in surgical bed, it extends
from the subphrenic region to the flank, with approximate dimensions of
20 x 9 x 7.8 cm, with a 730 cc estimated volume. The hematoma had
heterogeneous density ranging from 20 to 66 HU, due to different stages
of bleeding
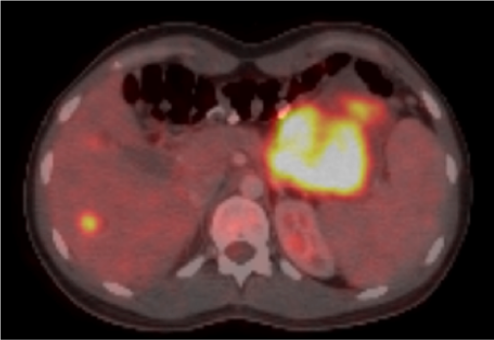
Figure 3. The liver presented multiple hypodensity lesions in segments
V, VI, VII and VIII, the largest lesion on segment VI with 17 mm,
associated with an increased metabolism with a maximum SUV of 7.1 and
splenomegaly. No mesenteric, retroperitoneal adenopathy, iliac chains
or inguinal were identified

Figure 4. Product of the distal pancreatectomy with splenectomy